
CALL US NOW
079 - 26400979

QUICK INQUIRY
contact@jointcarearthroscopy.com
The rotator cuff muscle is a prime muscle in stabilizing the shoulder joint & allows us to lift the arm above the head. Due to wear & tear over time it is common in patients above age of 50 years to develop a rotator cuff tear. Often this tear occurs without any fall or trauma. However, sometimes due to prevailing degeneration within the rotator cuff a trivial trauma – such as fall in bathroom or at times even after a throwing injury. Patients complain of pain at the side of the arm and inability to actively lift the arm.
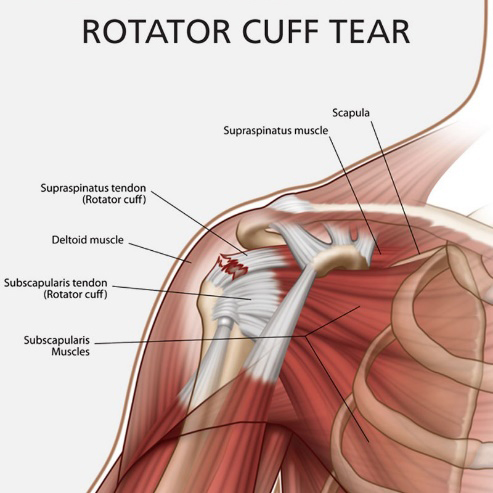
The term “Rotator Cuff” is used to describe the group of muscles and their tendons in the shoulder that helps control shoulder joint motion. The supraspinatus is at the top (superior) of the shoulder, the Subscapularis is anterior (front), and the infraspinatus and Teres minor are posterior (behind). These muscles insert or attach to the humeral head by way of their tendons. The tendons fuse together giving rise to the term “cuff.” Although each muscle acting alone may produce an isolated rotational movement of the shoulder, the role they play together is to help keep the humeral head (ball) centered within the glenoid (socket) as the powerful deltoid and other larger shoulder muscles act to lift the arm overhead.
The muscles and tendons in the rotator cuff group may be damaged in a variety of ways. Damage can occur from an acute injury (for example from a fall or accident), from chronic overuse (like throwing a ball or lifting), or from gradual degeneration of the muscle and tendon that can occur with aging.Rotator cuff pathology can be caused by extrinsic (outside) or intrinsic (from within) causes. Extrinsic examples include a traumatic tear in the tendon(s) from a fall on out stretched hand or accidents. Overuse injuries from repetitive lifting, pushing, pulling, or throwing are also extrinsic in nature which tear tendons even with trivial or no injury. Intrinsic factors include poor blood supply, normal attrition or degeneration with aging, and calcific invasion of the tendon(s). Usually in young individuals significant extrinsic trauma and in older individuals more of intrinsic factors making cuff tendons so weak that even trivial or no trauma leads to cuff tears. That is the reason that in older individual sometimes cuff tears are asymptomatic.
Rotator cuff “tendonitis” is the term used to describe irritation of the tendon(s) either from excessive pressure on the acromion or less commonly from intrinsic tendon pathology. Irritation of the adjacent bursa is known as Subacromial “bursitis.” Repetitive overhead activities resulting in irritation of the tendon(s) and bursa from repeated contact with the under surface of the acromion is called “Impingement Syndrome.”
With a rotator cuff tear, you may experience pain primarily on top and in the front of your shoulder. Sometimes, pain may occur at the side of your shoulder, and it is usually worse with any activity that forces you to reach above the level of your shoulder. You may also experience weakness and stiffness, and it may be difficult to perform simple overhead activities like placing dishes in the cupboard. Some people with tears can’t lift their arm to comb their hair. Stiffness may result from the inability to move your shoulder, and this stiffness may become progressive.
Often with a rotator cuff tear, bursitis (inflammation of the bursa, the small sac of fluid that surrounds the joint) will occur, which may cause a mild popping or crackling sensation in the shoulder. The tear itself may rub and cause this sensation. You may also have difficulty sleeping on the shoulder at night.
X-rays will not show the rotator cuff, but they will reveal any evidence of arthritis, spurs within the shoulder, loose bodies, fractures from a related fall, abnormal displacement of the humerus out of the glenoid, and congenital (birth) related problems. Therefore, good quality x-rays are a must in the proper evaluation of the shoulder.
Ultrasound examination is good tool to rule out actual significant rotator cuff tear as a screening process but it is dependent on the quality and specificity of machine and experience of the radiologist. The MRI scan is mandatory for the operative treatment plan of the rotator cuff tear.
Magnetic Resonance Imaging or MRI has allowed visualization of the soft tissues of the body, including the rotator cuff. An MRI can depict tendonitis, partial tearing, and complete tears of the rotator cuff. While an MRI is usually not required to diagnose a torn rotator cuff, it can be very helpful to determine which tendons are torn, how large the tear is, the degree of tendon retraction, the extent of muscle belly atrophy (shrinkage), and any coexisting problems.
If there is a partial tear this can be treated by our special shoulder rehab programme. But once a full thickness tear occurs it can only be treated by surgical repair. Without repairing the tear the shoulder cannot gain function. Local heat or physio does not address the cuff defect. The tear will propagate with time and the later a patient presents the poorer the outcome. Some patients have to be refused surgery as they present too late.
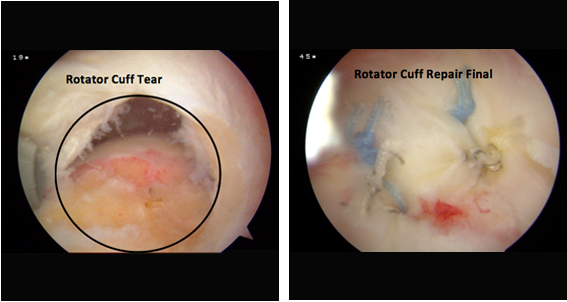
Traditionally rotator cuff used to be repaired with open surgery leading to adhesions and post operative stiffness & recovery generally takes a very long time. At our hospital rotator cuff is repaired arthoscopically with the use of imported suture anchors. After arthroscopic repair, patients go home the next day of surgery & with hardly any scar. Also, working patients tend to join back work within a week of surgery. Patients presenting late will tend to have a poor quality of muscle to repair.
Typically patients are admitted the evening before surgery or in the morning on the day of surgery.
Certainly avoid smoking for a week before surgery and six weeks after surgery. Nicotine has an adverse effect on General anesthesia. Smoking also retards healing of tissue and re-tear rates are higher in smokers. Avoid alcoholic drinks a day before and after surgery as alcohol counteracts with your medication. It is desirable to have a bath before surgery.
rotator cuff repair is a major operation that requires considerable rehabilitation. Several rehabilitation protocols for rotator cuff repair are available and are based on the size of the tear and repair. The shoulder is typically protected in a sling for 4 to 10 weeks, although some gentle passive motion is typically begun almost immediately.
It takes 12 weeks for the tendon to begin to heal down to the bone, and that the attachment continues to mature and strengthen for 2 years. Despite the prolonged healing course, patients can very often begin light computer work or writing in 6 weeks, lift the arm overhead 2 to 4 months after surgery depending upon type and health of cuff tissue. Participate in household work table work & other less strenuous activities at 4 months, and return to full sports and work participation at 6 to 8 months.
Long term studies have revealed 80 to 95 percent good to excellent results for rotator cuff repair done r arthroscopically. Patient satisfaction rates are high. In the majority of these studies, over 90% of patients agreed that in retrospect they would have the surgery again if needed. A well-motivated patient combined with a well-done repair and a comprehensive rehabilitation program, typically results in a satisfied patient who is able to return to his or her normal activities of daily living with little to no compromise.

 I am very thankful to Dr. Chirag Chudasama who made me to play again my dream sports. I was unable to do balling and fielding on boundary. Throwing ball was such a painful like a hell. I used to ply cricket for polo club at Baroda in under 20 team and even...
I am very thankful to Dr. Chirag Chudasama who made me to play again my dream sports. I was unable to do balling and fielding on boundary. Throwing ball was such a painful like a hell. I used to ply cricket for polo club at Baroda in under 20 team and even...


4th Floor, Dev Complex, Parimal Garden Cross Roads, C.G. Road,
Ahmedabad-380006
 079 - 26400979
079 - 26400979 




