
CALL US NOW
079 - 26400979

QUICK INQUIRY
contact@jointcarearthroscopy.com
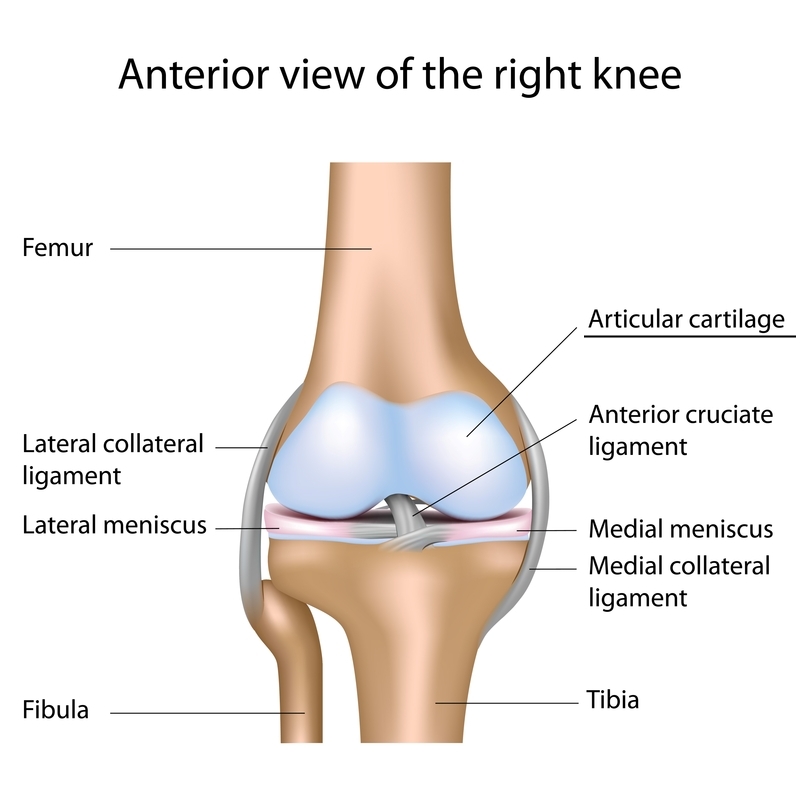
the body: articular or hyaline cartilage (covers joint surfaces), fibrocartilage (knee meniscus, vertebral disk), and elastic cartilage (outer ear). These different cartilages are distinguished by their structure, elasticity, and strength. In some joints, such as the knee, both articular cartilage and fibrocartilage are found functioning side-by-side as distinctly different structures with different functions. When the meniscus is injured, it is sometimes referred to as “torn cartilage” or “torn meniscus.” This is different than joint surface articular cartilage problems discussed here. Articular cartilage is a complex, living tissue that lines the bony surface of joints. Its function is to provide a low friction surface enabling the joint to withstand weight bearing through the range of motion needed to perform activities of daily living as well as athletic endeavours. Those daily activities include walking, stair climbing and work-related activities. In other words, articular cartilage is a very thin shock absorber. It is organized into five distinct layers, with each layer having structural and biochemical differences.
the body: articular or hyaline cartilage (covers joint surfaces), fibrocartilage (knee meniscus, vertebral disk), and elastic cartilage (outer ear). These different cartilages are distinguished by their structure, elasticity, and strength. In some joints, such as the knee, both articular cartilage and fibrocartilage are found functioning side-by-side as distinctly different structures with different functions. When the meniscus is injured, it is sometimes referred to as “torn cartilage” or “torn meniscus.” This is different than joint surface articular cartilage problems discussed here. Articular cartilage is a complex, living tissue that lines the bony surface of joints. Its function is to provide a low friction surface enabling the joint to withstand weight bearing through the range of motion needed to perform activities of daily living as well as athletic endeavours. Those daily activities include walking, stair climbing and work-related activities. In other words, articular cartilage is a very thin shock absorber. It is organized into five distinct layers, with each layer having structural and biochemical differences.
Articular cartilage injuries can occur as a result of either traumatic mechanical destruction, or progressive mechanical degeneration (wear and tear). With mechanical destruction, a direct blow or other trauma can injure the articular cartilage. Depending on the extent of the damage and the location of the injury, it is sometimes possible for the articular cartilage cells to heal. Articular cartilage has no direct blood supply, thus it has little or no capacity to repair itself. If the injury penetrates the bone beneath the cartilage, the underlying bone provides some blood to the area, improving the chance of healing. Occasionally an articular cartilage fragment completely breaks loose from the underlying bone. This chip, called a loose body, may float in the joint interfering with normal joint motion. Mechanical degeneration (wear and tear) of articular cartilage occurs with the progressive loss of the normal cartilage structure and function. This initial loss begins with cartilage softening then progresses to fragmentation. As the loss of the articular cartilage lining continues, the underlying bone has no protection from the normal wear and tear of daily living and begins to
break down, leading to osteoarthritis. Also known as degenerative joint disease, osteoarthritis is characterized by three processes:
In many cases, a patient will experience knee swelling and vague pain. At this point continued activity may not be possible. If a loose body is present, words such as “locking” or “catching” might be used to describe the problem. With mechanical degeneration (wear and tear), the patient often experiences stiffness, decreased range of motion, joint pain and/or swelling.
The physician examines the knee, looking for decreased range of motion, pain along the joint line, swelling, fluid on the knee, abnormal alignment of the bones making up the joint and ligament or meniscal injury. Injuries to the articular cartilage are difficult to diagnose, and evaluation with MRI (magnetic resonance imaging) or arthroscopy may be necessary. Plane X-rays are not usually good in diagnosing articular cartilage problems but are usually taken to rule out other abnormalities.
When a joint is injured, the body releases enzymes that may further break down the already damaged articular cartilage. Injuries to the cartilage that do not extend to the bone will generally not heal on their own. Injuries that penetrate to the bone may heal, but the type of cartilage that is laid down is structurally unorganized and does not function as well as the original articular cartilage. Defects smaller than 2 cm have the best prognosis and treatment options. Those options include arthroscopic surgery using techniques to remove damaged cartilage and increase blood flow from the underlying bone (e.g. drilling, pick procedure). For smaller articular cartilage defects which are asymptomatic, surgery may not be required. For larger defects, it may be necessary to transplant cartilage from other areas of the knee (joint).
Anti-inflammatory medication or systemic steroids can be taken to decrease inflammation. These systemic treatments can affect the entire body, not just the involved joint. They are helpful when the patient has generalized inflammation, such as inflammatory arthritis (rheumatoid arthritis) or multiple joint aches. Ice or cryotherapy can also be used to decrease swelling of the joint. Cool temperature leads to decreased inflammation and lower cellular activity and can decrease symptoms. When icing the joint, it is important to keep the put a layer of cooling device or ice.
Corticosteroid injection directly into the joint can be used to suppress inflammation and thus, decrease pain. Other injections, such as hyaluronic acid, can also be used. The latter are also known as artificial joint fluid injections, which are products that have similar composition to human synovial fluid. These can act as lubricants for the knee and decrease swelling or irritation. However, the injection itself does not treat the underlying condition. Unstable cartilage or loose cartilage fragment can still lead to persistent swelling after the effect of the injections has worn off. The effect of injections is dependent on the severity of the problem. It normally takes 2-3 days to come into effect and may last up to weeks and months.
Cartilage injuries or unstable cartilage can be treated surgically. Most surgical procedures are recommended for high grade cartilage injuries that require resurfacing or debridement. For debridement, the unstable cartilage is removed using an arthroscopic shaver, after which resurfacing can be performed in a variety of ways.
Articular cartilage is biopsied or taken from the patient’s knee during arthroscopic surgery. The chondrocytes from the cartilage are then isolated and grown in the laboratory over a 6-8 week period. After a sufficient number of chondrocytes has been cultured, they are injected back into the defect of the knee, where a periosteal flap covers the defect. This technique is the first cell-based type treatment of cartilage injuries. The initial advancement has led to significant amount of interest, however, the long-term results of ACI are still unknown?. Nonetheless, this technique has opened doors for significant development and hopefully, better methods of implanting cultured cells.
In general, joint replacements are reserved for end-stage cartilage injuries and older patients. Newer designs and improved bearing surfaces will likely lead to longer durability of the implants, and may improve long-term success rates.

 I am very thankful to Dr. Chirag Chudasama who made me to play again my dream sports. I was unable to do balling and fielding on boundary. Throwing ball was such a painful like a hell. I used to ply cricket for polo club at Baroda in under 20 team and even...
I am very thankful to Dr. Chirag Chudasama who made me to play again my dream sports. I was unable to do balling and fielding on boundary. Throwing ball was such a painful like a hell. I used to ply cricket for polo club at Baroda in under 20 team and even...


4th Floor, Dev Complex, Parimal Garden Cross Roads, C.G. Road,
Ahmedabad-380006
 079 - 26400979
079 - 26400979 




